Management and Treatment
Standard treatment to control blood cell count (cytoreductive therapy) in polycythaemia vera is hydroxycarbamide or interferon alfa.
Ruxolitinib would be used for people who cannot tolerate hydroxycarbamide or when the condition is resistant to it.
Results from clinical trials suggest that ruxolitinib is more effective than standard treatment at controlling blood cell counts and reducing spleen size. But whether it increases how long people live is uncertain.
Because of the uncertainty in the clinical-effectiveness evidence, the cost-effectiveness estimates need to be towards the lower end of the range that NICE considers an acceptable use of NHS resources. They are below this lower end, so ruxolitinib is recommended.
Newer Treatments
The latest treatments for polycythemia vera (PV) focus on improving disease management and reducing complications. Here are some of the most recent advancements:
1. Ropeginterferon alfa-2b (Besremi): This is a novel pegylated interferon approved as a first-line treatment for PV in the EU. It has shown higher hematological and molecular response rates compared to hydroxyurea and is better tolerated than other types of interferon-α[1].
2. Rusfertide: This is an injectable synthetic medication administered once a week that has demonstrated effective hematocrit control in PV patients. It can be used alone or in combination with other treatments[2].
3. Ruxolitinib (Jakafi): This JAK2 inhibitor is approved as a second-line treatment for PV patients who are intolerant or have an inadequate response to hydroxyurea[3].
4. Givinostat: This histone deacetylase medication is being studied as a potential second-line treatment for patients who don't tolerate first-line therapies well[4].
5. Pegylated interferon alfa-2a (Pegasys): Another JAK2 inhibitor targeting the JAK2 gene, which may benefit PV patients[4].
6. Idasanutlin: An MDM2 inhibitor that blocks certain protein interactions, although it may not be suitable for long-term use[4].
In addition to these newer medications, standard treatments still play a crucial role:
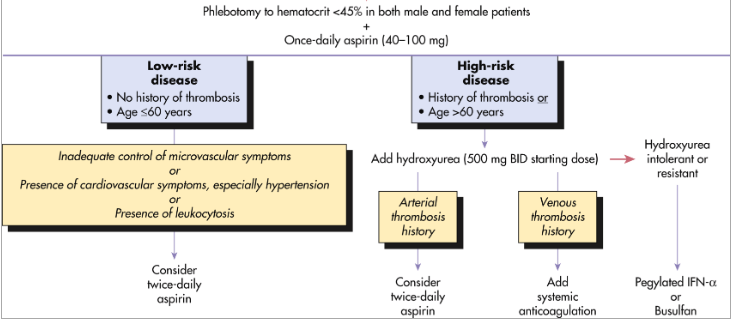
- Phlebotomy (blood withdrawals) remains the most common treatment for reducing blood volume and excess blood cells[3].
- Low-dose aspirin is often prescribed to reduce the risk of blood clots[3].
- Hydroxyurea is still used as a first-line cytoreductive therapy in some cases[1].
It's important to note that treatment strategies are individualized based on the patient's risk factors, age, and specific symptoms. The goal of these treatments is to reduce the risk of complications, particularly thrombosis, and improve quality of life for PV patients[1][3][4].
Citations:
[1] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10701315/
[2] https://www.targetedonc.com/view/new-agents-advance-treatment-options-for-polycythemia-vera
[3] https://www.mayoclinic.org/diseases-conditions/polycythemia-vera/diagnosis-treatment/drc-20355855
[4] https://www.medicalnewstoday.com/articles/latest-treatments-for-polycythemia-vera
[5] https://www.fda.gov/news-events/press-announcements/fda-approves-treatment-rare-blood-disease